Biomedicine
Characterization of adverse events during the treatment with heberprot-P® in four cuban provinces.
Caracterización de los eventos adversos reportados durante el tratamiento con Heberprot-P® en cuatro provincias de Cuba
Alina R. Alvarez CrespoI1, Liuba Alonso Carbonell2 , E , C Isis B. Yera Alós3, Dr. C Ana J. García Milián 4, Dr. C María Acelia Marrero Miragaya 5
(1) First Degree Specialist in Integral General Medicine. Master in Clinical Pharmacy. Assistant Professor. Investigator Attaché. Centro Nacional Coordinador de Ensayos Clínicos. Havana. alina@cencec.sld.cu.
(2) Second Degree Specialist in Pharmacology. Master in Health Promotion. Investigator and Assistant Professor. Centro Nacional Coordinador de Ensayos Clínicos. Havana. liuba@cencec.sld.cu o.
(3) Stomatologist. Doctor of Health Science. Second Degree Specialist in Biostatistics. Master in Health Economics. Investigator and Assistant Professor. Centro de Ingeniería Genética y Biotecnología. Havana. isis.yera@cigb.edu.cu .
(4) Medical Doctor. Doctor of Health Science. Second Degree Specialist in Pharmacology. Master in Health Economics. Investigator and Associate Professor. Escuela Nacional de Salud Pública. Havana. purmed@infomed.sld.cu .
(5) Medical Doctor. Doctor of Health Science. First Degree Specialist in Surgery. Investigator and Assistant Professor. Centro Nacional Coordinador de Ensayos Clínicos. Havana. acelia@cencec.sld.cu
Original article received july 9, 2015
Approved august 10, 2015
CORRESPONDING AUTHOR: Ana Julia Garcia Milian. Escuela Nacional de Salud Pública. La Habana. E-mail. purmed@infomed.sld.cu
Abstract
Objective. The objective of this study and the reason that encouraged us to carry out this work was to characterize the adverse events reported during the treatment with Heberprot-P® in different health institution/ centers. Materials and Methods: Longitudinal, multicenter, postmarketing follow-up study of Heberprot-P®. Intensive surveillance was used as PS (pharmacosurveillance) method. The following variables were considered: presence or absence of AEs (adverse events); most frequently reported AEs; affected organ system; serious AE according to cause conditioning both the event severity and type, and severity of ADRs (adverse drug reactions) and causality of AE reported as serious. Results: The presence of at least one AE was reported in 260 patients (59.1%). Burning sensation and pain in injection site, chills and shivering, were the four most frequently reported adverse events. A total of 11 events were identified as serious. Conclusions: The intensive PS of the drug should be continued since all the routine medical practice data that could be contributed are essential for the purpose of enriching the drug's safety profile.
Keywords: Adverse drug reaction, Pharmacosurveillance, Diabetic foot ulcer.
Resumen
Objetivo: Caracterizar los eventos adversos reportados durante el tratamiento con Heberprot-P® en diferentes instituciones de salud fue el objetivo del estudio y lo quenos motivó a efectuar éste trabajo. Materiales y metodos: Estudio longitudinal y multicéntrico de seguimiento post-comercialización de Heberprot-P® y se empleó como método de FV, la vigilancia intensiva. se utilizaron las variables siguientes: Presencia o no de EA, EA más frecuentes reportados, sistema de órganos afectado, EA grave según motivo que condicionó la gravedad del evento y tipo de evento y la gravedad de las RAM y causalidad del EA reportado como grave. Resultados: En 269 pacientes (59,1%) se reportó la presencia de al menos un EA. El ardor y el dolor en el sitio de inyección, las tiriteras y los escalofríos fueron los cuatro eventos que más reportes presentaron. Se determinaron como graves 11 eventos. Conclusiones: Se debe continuar la FV intensiva del fármaco, ya que son necesarios todos los datos que se aporten en las condiciones de la práctica médica habitual, con la finalidad de enriquecer el perfil de seguridad del mismo.
Palabras claves: Reacción Adversa a Medicamento, Farmacovigilancia, Úlcera de Pie Diabético.
Introduction
Medications are the medical technology most frequently used currently. Their development has modified the manner in which diseases are prevented and treated, favoring changes in their epidemiological profile in various regions of the world. However, despite the advantages they offer, there is increasing evidence that adverse drug reactions (ADRs) are a frequent, though often preventable cause of disease, disability, or even death, to the point of being included on the list of the 10 main causes of death in some countries.1
The surveillance of medication safety can potentially promoting inspire trust in regards to their use in both patients and health care professionals, while being regarded as an essential element to achieve a safe use of drugs and high-quality medical care.
Post-marketing investigations with biological and biotechnological products are a challenge in the sense that their effectiveness and safety may be affected by several factors, such as the molecular structure complexity, heterogenicity of molecular composition, sensitivity to changes in physical conditions, and immunogenicity, hence the need for a comprehensive pre-clinical and clinical program and an adequate postmarketing pharmacosurveillance (PS).2,3
The Centro para el Desarrollo dela Farmacoepidemiologia (Center for Pharmaco-epidemiology Development) (CDF, for its acronym in Spanish) undertook the responsibility for performing the follow-up of Heberprot-P®, as requested and under contract with the Centro de Ingeniería Genética y Biotecnología (Genetic Engineering and Biotechnology Center) (CIGB, for its acronym in Spanish) for the purpose of determining its effectiveness, identifying and quantifying its adverse events (AEs), particularly those not known before its registration, and determining possible risk factors or effect modifies, as well as knowing the effects of the drug from the perspective of patients in non-controlled situations of regular clinical practice.
A Heberprot-P® is prescribed for the treatment of diabetic foot ulcer (DFU). In previous phase I, II, and III clinical trials, the intralesional administration of the drug was shown to mitigate the consequences of neurogenic ischemia and protect peripheral soft tissues, as well as to contribute to the formation of granulation tissue and favoring its healing action, effect that is associated to a reduction in the number of amputations. 4
The medication was introduced to the Cuban Basic Schedule of Essential Drugs in April 2007. From that date on, an expansion strategy was started in the Sistema Nacional de Salud (National Health System) (SNS, for its acronym in Spanish), aimed at implementing its use and integral management for DFU in all the diabetic patient care services/centers.5
Characterizing the adverse events reported during the treatment with Heberprot-P® in various healthcare institutions was the objective of this study and the reason that encouraged us to carry out this work.
Materials and Method
An observational, analytical, prospective, longitudinal, multicenter study Heberprot-P® post-marketing followup was carried out, using an intensive surveillance as PS method.
The study was undertaken in the period stretching from June 2007 to March 2010, after the national expansion of Heberprot-P® in the SNS. All Cuban patients of any sex, aged 18 or over, and with clinical diagnosis of DFU of different Wagner grades6 , were considered eligible and received the product at healthcare institutions in the provinces of Pinar del Rio, Havana, Havana City and Matanzas. The study group comprised 455 patients. Individuals with non-compensated chronic diseases, history of or suspected malignant diseases, hypersensitivity to the product or any of its components, pregnant or lactating, or with ulcers affecting an area < 1 cm2 were excluded. The criteria considered included cessation of treatment, overgranulation of lesion, voluntary withdrawal, presence of serious AE, extension of ulcerative area, and indication of major amputation.
In order to fulfill the specified objective, the following variables were used: presence or absence of AEs; most frequently reported AEs; affected organ system; serious AEs according to the type of event and cause that conditioned severity, and existing causality relationship of the various AEs reported as serious.
To evaluate the causality of ADR reports, the most frequently used method is the qualitative and quantitative algorithm of Karch and Lasagna, relating 5 categories: definite, probable, possible, conditional, and non related, and refers to the casual relationship between drug treatment and the occurrence of adverse reactions in the case of individual suspected ARs.7
Besides causality, the magnitude of the adverse event effect on an individual is also related to the severity of the AE which can then be classified according the World
Health Organization (WHO) as mild, moderate, severe of fatal, depending on whether it affects or not and to what degree the activities of daily living.8
The assessment of severity requires an individualized study of the adverse event, as well as of the reaction duration and intensity.
Another classification used is the one relating results and their consequences, which can be serious or non serious. The categories were established on the basis of the classification of ADR severity by the WHO.7
Events were classified according to their severity and causality for serious AEs pursuant to the provisions set forth by the Standards and Procedures of the Cuban pharmacosurveillance system. The extent of organ system involvement was determined in accordance to the WHO terminology dictionary, 2008 edition.10
The serious AEs were reported within 24 hours to the provincial pharmaco-epidemiologist who, in turn, notified the CDF. The case was discussed first in each province by the provincial PS commission and then by a group of experts established for the purpose of this investigation and that comprised specialists in angiology and vascular surgery, cardiologists, clinicians, qualified staff from the PS department of the CIGB and CDF investigators, all of whom had access to the postmarketing study.
The variables related to safety were subjected to descriptive analysis. The reporting frequency of AEs was calculated taking as denominator the total of patients exposed to intensive surveillance during the study period.
A data entering model was designed to collect all the necessary information that was later transferred to a database created in the Statistical Package for Social Sciences (SPSS), Version 11.5, with the information from the corresponding data collection logbooks.
Information was presented in tabular form
Results
The presence of at least one AE was reported in 269 patients (59.1%). In total, 1,527 events were reported and grouped into 48 different types. Of these, 92.4% (1,411) were classified as mild and 6.9% (105) as moderate. Burning sensation and pain the injection site, chills and shivering, were the most frequently reported adverse events (see Table 1).
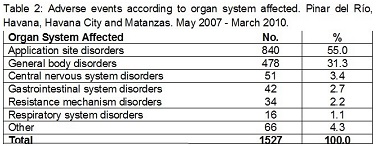
The most frequently involved organ system was the application site (55.0%), followed by general body disorders (31.3%) (Table 2).
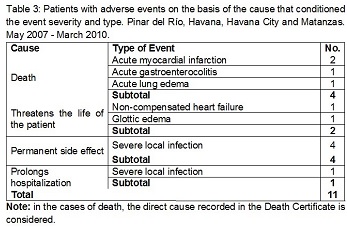
A total of 11 adverse events were classified as serious (0.7%) that correspond to the same number of patients, four of which had a fatal outcome and seven were either life threatening, led to permanent sequels or prolonged the patient hospitalization (see Table 3).
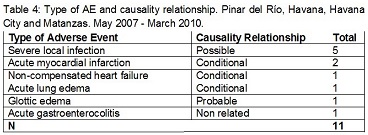
Of the 11 reported AEs, 5 were classified as possible, 4 as conditional, 1 as probable and the remaining one as non related (see Table 4).
Discussion
The most frequent AEs correspond to those reported in the clinical essays (CEs) developed for the product 4 and in post-marketing studies.11, 12, 13
During the previous clinical essays, pain and burning sensation on the application site are reported as related to administration method. Besides, chills and shivering where the only AEs where a definite or probable dose-dependent causal relationship was found with the use of Heberprot-P®. A pyrogenic reaction was ruled out because the product is released as "free of pyrogens" specification. It is possible to speculate whether the epidermal growth factor (EGF), at the drug concentrations reached after the intralesional administration, may interact with the thermoregulatory centers in the hypothalamus, in the same manner that other cytokines do. A direct action of EGF on the SNS has been reported after its intraventricular injection.
The types of reported events and the product administration method conditioned that the most affected system organs were the application site, followed by general body disorders. Similar results were described by other authors.11, 15, l6, 17, 18
Dominguez Caballero10 and Ramirez Calzadilla in investigations conducted in other provinces of the country, reported a profile of serious AEs similar to the In the causality analysis, events such as myocardial infarction, non-compensated heart failure, and acute lung edema were classified as conditional. The literature on the subject indicates that diabetes mellitus is one of the major risk factors for cardiovascular diseases,20 21 22 23 and the presence of DFU adds an additional risk, both in terms of general mortality as well as mortality due to an acute myocardial infarction.22
To provide an adequate and correct judgment on this matter, more data were needed.
A possible causality relationship was attributes to local infection, since it represents one of the most frequently reported serious events in the clinical essays of this product. This event may also be explained by the basic disease of the patient and the disease that cause the product to be administered (DFU).
Glottic edema associated to dyspnea, erythrocianosis, and mild precordialgia was considered as probable since it was a reasonable temporary side effect related to the drug administration (single dose) and it unlikely to be attributed to the concurrent disease. The patient was receiving a treatment with ceftazidime, but the temporary relationship was feasible with the administration of Heberprot-P®.
Acute gastroenterocolitis was classified as related since it occurred in a patient and the time sequence between the event and the last administration of the drug, did not justify its occurrence and could be explained by the underlying disease.
Heberprot-P® was recently launched in the market and some of these AEs are not mentioned in the product information.24
Conclusions
The PS of the medication should be continued since all the data are needed that contribute to the conditions of physicians' daily medical practice, with the aim of improving the knowledge on its safety profile.
References
1. Organización Mundial de la Salud. La farmacovigilancia: garantía de la seguridad en el uso de los medicamentos. Perspectiva política de la OMS sobre medicamentos. Ginebra: OMS; 2004.
2. Laporte J.R. El Ensayo Clínico Controlado. En: Principios básicos de la investigación clínica. 2da ed. Barcelona: Astra Zeneca; 2001: 28-51.
3. Marletta L. Aspectos Regulatorios de los productos biológicos/biotecnológicos, Argentina 2008. [Citado 30 de mayo de 2015]; available in: http://www.ebebiopharma.org/forcedownload.php?file=/media/ biosimilars/biosimilar
4. Fernández-Montequín JI, Infante-Cristiá E, Valenzuela-Silva C, Franco-Pérez N, Savigne-Gutierrez W, Artaza-Sanz H, et al. Intralesional injections of Citoprot-P_ (recombinant human epidermal growth factor) in advanced diabetic foot ulcers with risk of amputation. Int Wound J. 2007; 4:333-343.
5. Colectivo de autores. Experiencia Cubana en la extensión del uso del Heberprot -P. En: Fernández-Montequín J, Berlanga Acosta J, López Saura PA, López Mola E, Herrera ML, Yera Alós I, et al. Infiltración del Heberprot-P. La Habana. Ed. Elfos Scientiae; 2009:100-106.
6. Oyibo SO, Jude EB, Tarawneh I, Nguyen HC, Harkless LB, Boulton AJ. A comparison of two diabetic foot ulcer classification systems: the Wagner and the University of Texas wound classification systems. Diabetes Care 200i;24(1):84-88.
7. Karch FE, Lasagna L. Toward the operacional identification of adverse drug reactions. Br J Clin Pharmacol 1977; 21(3)247-254.
8. Armijo J, González Ruiz M. Estudios de seguridad de medicamentos: Métodos para detectar las reacciones adversas y valoración de la relación causa-efecto. En: El ensayo clínico en España. 2002; 161:190.
9. Centro para el Desarrollo de la Farmacoepidemiología. "Normas y procedimientos de trabajo del sistema cubano de farmacovigilancia".2007. [Citado 30 de mayo de 2015]. available in: http://www.cdf.sld.cu/fv/NormasyProcedimientos2007.htm.
10. Uppsala Monitoring Centre. 2010 October[Citado 30 de mayo de 2015]; available in: http://www.who-umc.org.
11. Domínguez Caballero JL. Evolución clínica y seguridad del Factor de Crecimiento Epidérmico Humano Recombinante en pacientes tratados en las provincias centrales Cuba 2007-2009" [tesis]. Centro para el Desarrollo de la Farmacoepidemiología; 2010.
12. Llanes Barrios JA; Fernández Montequín JI; Seuc AH; Chirino Carreño N; Hernández Rivero MJ. Caracterización del pie diabético y algunos de sus factores de riesgo. Rev Cubana Ang Cir Vasc [serial on the Internet]. 2010 [Citado 15 de enero de 2015]; 13(2): [p.10-18] Available in: http://bvs.sld.cu/revistas/ang/voln_01_10/ang02110.pdf
13. Hernández Rivero MJ, Llanes Barrios JA, Acosta Lapera DS. Heberprot-P, una terapia eficaz en la prevención de la amputación en el pie diabético. Rev Cubana Ang Cir Vasc [serial on the Internet]. 2009 [Citado 15 de enero de 2015]; 10(1): [p. 3-11] Available in: http://bvs.sld.cu/revistas/ang/vol10_1_09/ang02109.pdf
14. Kushikata T, Fang J, Chen Z, Wang Y, Krueger JM. Epidermal growth factor enhances spontaneous sleep in rabbits. Am J Physiol 1998; 275:509-514 1 chronic diabetic foot ulcer: treatment up to complete wound closure. Int Wound J. 2009; 6(1)67-72.
15. Fernández-Montequín JI, Betancourt BY, Leyva-González G, López Mola E, Galán-Naranjo K., Ramírez-Navas M, et al. Intralesional administration of epidermal growth factor-based formulation (Heberprot-P) in chronic diabetic foot ulcer: treatment up to complete wound closure. Int Wound J. 2009; 6(1):67-72.
16. Gil RM, López Mola E, Álvarez H, Hernández A, Pérez C, Yera I, et al. Experiencias en la extensión nacional del programa de atención integral al paciente con úlcera del pie diabético y el empleo del Heberprot-P. Rev Biotec Aplic. 2010;27(2):142-146.
17. González Acosta S, Calaña González-Posada B, Marrero Rodríguez I, López Fernández R. Evolución clínica del tratamiento en el pie diabético con Heberprot-P o con el método convencional. Rev Cubana Ang Cir Vasc [serial on the Internet]. 2011 [Citado 15 de enero de 2015]; 11(2): [8 p.] Available in: http://bvs.sld.cu/revistas/ang/vol_11_2_11/ang07211.htm
18. Velázquez W, Valles A, Curbelo W. Impacto del Heberprot-P® en el tratamiento de las úlceras de pie diabético. Rev Biotec Aplic. 2010; 27(2)129-135.
19. Ramírez Calzadilla Y. Evolución clínica y seguridad del Factor de Crecimiento Epidérmico Humano Recombinante en pacientes tratados en Holguín, Granma y Santiago de Cuba. Cuba. 2007-2009" [tesis]. Centro para el Desarrollo de la Farmacoepidemiología; 2010.
20. Grossman E, Messerli FH. Diabetic and hypertensive heart disease. Ann Intern Med 1996; 125:300-310.
21. Crespo Mojena N, Martínez Hernández A, Rosales González E, Crespo Valdés N, García Roura J. Diabetes mellitus e hipertensión: Estudio en el nivel primario de salud. Rev Cubana Med Gen Integr [revista en la Internet]. 2002 Oct [Citado 15 de enero de 2015]; 18(5):331-335.available in: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252002000500007&lng=es.
22. Mor Bach S, Lutale JK, Viswanathan V. Regional differences in diabetic foot lesions. Diabet Med 2004; 21(1): 81-85.
23. Campbell PT, Newton CC, Patel AV, Jacobs EJ, Gapstur SM. Diabetes and cause-specific mortality in a prospective cohort of one million U.S. adults. Diabetes Care 2012; DOI: 10.2337)12-0002.
24. Centro para el Desarrollo de la Farmacoepidemiología. Formulario Nacional de Medicamentos. Información del producto Heberprot-P. La Habana: Ciencias Médicas; 2006. [Citado 15 de enero de 2015]; Available in: http://fnmedicamentos.sld.cu/index.php?P=FullRecord&ID=648