Public Health
Social perception of childhood overweight and obesity to generate prevention strategies in Nuevo León, Mexico
Percepción social del sobrepeso y la obesidad infantil para la generación de estrategias de prevención
Janet García González1, Esteban Picazzo Palencia2, Dora Elia Cortes Hernández3, Kabáh Silva Aguilar 4
(1) Doctor of Communication, Specialist in Public Health and Epidemiology, Professor and Researcher, Universidad Autónoma de Nuevo León.
(2) Doctor in Social Sciences, Professor and Researcher, Universidad Autónoma de Nuevo León.
(3) Doctor in Public Health; Professor and Researcher, Universidad Autónoma de Nuevo León.
(4) Program, Universidad Autónoma de Nuevo León.
Original received June 11, 2015
Accepted August 11, 2015
CORRESPONDING AUTHOR: Janet García González, Aldebaran No 93, Paseo del Country, Monterrey, Nuevo León. México. CP 64860. E-mail: janetgarcia71@yahoo.com.mx
Abstract
Objective. To determine the social perception on childhood overweight and obesity for the purpose of generating communication strategies that would prevent it through changes in behavior. Materials and methods : A descriptive study using a qualitative research method that involved focus groups with children, teachers and parents. The type of analysis was argumentative. The study was conducted from January to May 2013 in the metropolitan area of Monterrey, Nuevo León, Mexico.
Results: There is a most different social perception among focus groups on the quality of life and happiness of children, with parents and teachers referring to food in relation to children happiness when it is provided as a reward or to compensate for bad experiences or lack of emotional attachment, while children refer to family harmony as the main cause for making them happy.
Conclusions: The social perception reveals the importance of social or symbolic interaction processes. Therefore, the objective of the communication strategy must address the associated factors in preventing obesity through symbolic elements of these groups, taking into account the senses and meanings related to basic stimuli that trigger behaviors related to obesity.
Keywords: social perception, prevention strategies, childhood obesity.
Resumen
Objetivo: Determinar la percepción social del sobrepeso y la obesidad infantil, para generar estrategias de comunicación en la intervención del cambio de la conducta para su prevención.
Material y métodos: Estudio descriptivo, método cualitativo y técnica de investigación fue grupos de discusión (niños, profesores y padres de familia). El tipo de anáisis fue argumentativo. Realizado de enero a mayo de 2013 en el área metropolitana de Monterrey, Nuevo León, México. Resultados: Existe una percepción social muy diferente en los grupos de discusión sobre la calidad de vida y felicidad de los niños; los padres y maestros hacen referencia hacia los procesos de atribución de la comida, como motivo de felicidad de estos a traves de recompensas y gratificaciones. Mientras que los niños, hacen alución que lo que los hace felices es la armonía familiar. Conclusión: La percepción social pone de manifiesto los procesos de interacción social y simbolica; para ello el objetivo de la estrategia de comunicación debe perseguir los factores asociados para la prevención de la obesidad con elementos simbólicos de los grupos, esto es, tomando en cuenta desde la percepción social los sentidos y significados que se relacionan con los estímulos básicos para desencadenar conductas relacionadas con la obesidad.
Palabras clave: percepción social, estrategia de prevención, obesidad infantil.
Introduction
At present, there exists a worldwide epidemic of non-communicable chronic diseases (NCCD), and obesity is one of the diseases classified under this heading.
Despite the call to action that has prevailed for more than one decade in the US, Europe and other developed countries, the obesity epidemic keeps on growing.1 Weight has increased since the XVII century in many of the countries that currently are part of the OECD, as the income, education, and life conditions gradually improved. Surveys started to record a considerable speeding up of the rhythm at which the body mass index (BMI) increased in the 80s, same index which grew two or three times faster in many countries versus the previous century.2 Though both the increase in size and BMI could have been considered as indicators of health improvements, the truth is that the pandemic growth of overweight and obesity has led to an opposite outcome, unleashing a number of public health issues.
The problem of obesity has broken down age barriers, and it Mexico it has turned into one of the most serious public health issues since the country now ranks first place in children obesity and second (only after the US) in adult obesity worldwide.3
Children obesity has negative consequences per se that influence adult morbidity and mortality, since childhood is the stage of life that will largely condition behavior in the adult age, as well as the development and persistence of obesity. In other words, it is more likely that overweight children would become overweight adults.4
Other data reinforce the severity of this problem among children. For example, the International Obesity Task Force (IOTF) estimated that 155 million children 1 to 10 years old suffered overweight or obesity. In the US, 9.6% of school-age children suffered obesity in the year 2000, and this figure was estimated to increase to 15.2% by 2010.5
Though obesity is a complex disease that is defined as an excess of body fat or fat tissue,6 it is process that usually starts in childhood or adolescence as a result of an unbalance between energy intake and expenditure. In its origin, there are genetic and environmental factors involved that determine a metabolic disorder which leads to an overaccumulation of body fat beyond the expected value for the specific sex, size and age.7
The environmental factors that determine obesity include the worldwide dietary change towards an increase in high-calorie foods, rich in fat and sugar, but poor in vitamins, minerals and other healthy micronutrients, as well as the trend to a reduction in physical activity due to the sedentary nature of most recreational activities, changes in transportation modes, and growing urbanization.8
Besides, the World Health Organization recognizes that the growing prevalence of children obesity is the consequence of social changes. Childhood obesity is fundamentally associated to a poor diet and limited physical activity, but the is not only related to the child's behavior, but also to social and economic development and to the policies in terms of agriculture, transport, urban planning, environment, education, and food processing, distribution and marketing.
To investigate the environmental agents that are involved in this disease, it must be taken into account that both school and family are the educational environments that have the greatest influence in developing eating habits and life styles that would strengthen along childhood and adolescence.9
Likewise, television (TV) is an environmental factor that has contributed decisively to the increased prevalence of childhood obesity, since spending long hours before the TV set also implies setting aside other activities that involve greater energy expenditure, the fact is that, if we take into account that children spend 990 hours annually sitting before electronic displays and only 960 hours at school, as shown by a study conducted in the autonomous regions by the Consell de l'Audiovisual de Catalunya, the influence of TV is more than evident on the physical inactivity of this population group or, to be more specific, the influence of advertising on the food intake trends of the child population.10
Besides, the advertising that is broadcasted and presented in-between TV children programs, turns the shows into advertising exhibitors aimed at stimulating the desire and need for consumption, in most cases, of foods that are rich in energy.9 The most used advertising strategies are promotions and association of food-stuffs to positive emotions, such as fun, happiness, games, fantasy, imagination, social integration and peer acceptance. Food advertising is more intense during the children's program time than in the prime time.11
All of the above plays a role in the problem, but the solution has focused in the implementation of health promotion programs and, at the local level, it is worth contextualizing the childhood obesity prevention strategies, since there are still limitations in terms of design, planning, and conduction of specifically oriented campaigns.12
In Mexico, the Secretary of Health, the Secretary of Public Education, the Mexican Institute of Social Security with its PREVENIMSS program, and some non-governmental organizations have launched advertising campaigns related to the increase of obesity, its co-morbidities, and serious effects on health, but they have not been enough.13 Despite their growing number, none of these campaigns has achieved the expected results since overweight and obesity are not determined only by the absence or deficiency of health system strategies, but by factors that arise from the social and economic environments, mainly.14
The three major objectives of public health are primary prevention, secondary prevention and damage control, and their role in the problem of obesity must be clearly identified. The National Health Institutes may contribute to it and help health programs to include the corresponding objectives. However, recognizing the need of obesity prevention is not enough since millions of Mexicans already suffer it. In general, adults are the decision-makers in regards to their family eating habits. Good strategies are needed for the treatment, control, and prevention of complications, and it must be acknowledged that a lot of creativity is needed to address this problem and identify possible solutions.15
Since the problem of obesity is a social one, it therefore requires a population, multisectorial, multidisciplinary approach that is adapted to the cultural circumstances. As opposed to the majority of adults, most children and adolescents choose neither the environment they live in, nor the foods they consume. Likewise, they have a limited ability to understand the long-term consequences of their behavior. Consequently, they need special care and monitoring in their struggle against obesity.16
I In the field of education, promotion, and social marketing, several common prevention messages such as that of "eat fruits and vegetables" that have not shown to generate the necessary impact.
"The effective communication of messages to the population does not depend solely on identifying the issues and in the knowledge of its determining elements, but also on the use of persuasion techniques similar to those used by the industry, and which require investment and a joint work between the associations of experts in the field and the promotion teams. "15
Hence, it is proposed that intuitive campaigns and "slogans" developed by the healthcare staff, as well as their entire concept of prevention, must be considered as the substrate for specialized creative groups to create the final population-targeted communications. Only then a similar impact and quality would be achieved as to those of advertising focused on the sale of products.
In conclusion, campaigns are needed which are aimed at raising awareness in the healthy, at risk, and even sick population, on the dangers of overweight and obesity and, equally, on the benefits of their control and prevention.13 However, to create an effective communication strategy on the prevention of this public health problem, a social perception diagnosis is needed regarding childhood obesity.
For the purpose of this study, it is worth mentioning that the meaning of social perception indicates that, belonging to a certain social class, involves a series of agents that directly or indirectly influence perceptual processes. These agents are related to the estimated wealth, environment, physical and mental development, education, etc.
Using the social psychology studies to justify the fact that campaigns on overweight and obesity prevention have not worked, it may be argued that no campaign has been prepared yet on the basis of social identity, same which is related to belonging to certain social categories or groups since, 11 from the perspective of symbolic interaction, all objects (in the sense given by Biumer (1969) to the term object) may include both all the spaces and social categories and acquire their ontological nature from the meanings conferred by individuals or groups," or in the words of Berger and Luckman (1966), "may be considered as social constructs".
In this sense, the statement of Stoetzel (1970) is particularly interesting: "The idea that the physical surrounding of an individual is entirely transcu tu red to the society he belongs to, and that describes the physical world, as perceived within a society and as object of adaptation to it, is equivalent to describing the culture of this society."1
Thus, it might be said that if communication is addressed as a social process of interaction and dissemination, an intervention mechanism can be created to generate a major social influence that provides knowledge, forges attitudes and triggers practices favorable for public health. It is on the basis of this proposal that this paper tries to determine the social perception of childhood overweight and obesity and, from it, to enable the development of intervention communication strategies to modify behaviors and enhance its prevention.
To achieve this purpose, a qualitative approach is used based on focus groups with strategic players, i.e., children, parents, and elementary school teachers since they have a direct relation with parents and with the environment in which children develop. This study was conducted in 2013 in the metropolitan area of Monterrey, Nuevo León, Mexico, and despite the fact that there are other researches regarding the perception of mothers on their children's body image,18 no evidence was found of an approach similar to the one proposed in this paper.
Material and methods
To carry out this study, a qualitative study was designed with focus groups and interaction analysis based on defined categories, hence accessing social knowledge through individuals and their behavior patterns.
The universe proponed for this research was the metropolitan area of Nuevo León, due to its serious obesity problem that affects approximately 25% of the children in Nuevo León, the highest percentage of obese children in the country.19
Three different groups were selected as targets for the focus groups:
1. Mothers. Since they are traditionall y responsible for preparing the foods for the entire family and supervising the children's food intake.
2. Teachers. Since their active contact with the children object of this study and their mothers makes of them an important study agent.
3. Children betwwen 6 and 12 years of age. To analyze the social discourse of the study object.
All the focus groups comprised 5 persons (criteria: uneven numbers, peers in similarity, homogeneous, not having met before). The contact was established at public schools, identifying those found in various socioeconomic areas of the metropolitan area of Monterrey. The invitation to participate was direct and the reason for the focus group and use to which information would be devoted were informed.
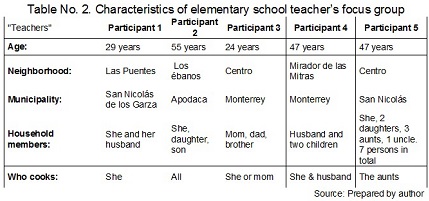
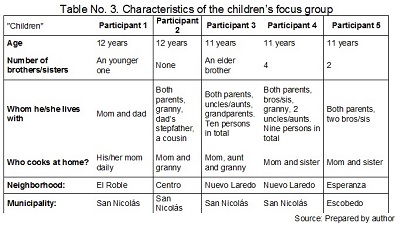
A data sheet was prepared of each focus group carried out which included the basic data of the participants. Their consent was given in oral fashion and through the signature of this data sheet. In total, nine focus groups were conducted, i.e., three different sessions for each interest group. A total of 45 individuals participated. Tables 1, 2 and 3 show an example of the characteristics of the focus groups:
The discussion subjects were built in each case according to the interventions of each participant. However, the moderator dominated over the group, assigned spaces and limited time using triggers for the each of the following semantic fields:
1. Children's quality of life conditions
1.1. Children's living conditions
1.2. Social structure of children
1.3. Children's life satisfaction
1.4. Childrens feeding
1.5. Most frequent eating places
2.Social perception of childhood obesity
2.1. Individual behavior regarding childhood obesity
2.2. Social behavior regarding childhood obesity
2.3. Perception of childhood obesity risks
2.4. Causes of childhood obesity
3.Social perception of eating
3.1. Eating
3.2. Junk food
4. Inflence of mass communication media on childhood obesity
4.1. Children consumption of mass communication media
4.2. Functional use of TV
4.3. TV programs consumed (watched) by children
The triggers were:
• Let's talk about how children live
• What makes children happy
• Food and children
• The places where children most frequently eat
• Obesity in children
• The risks of obesity in children
• Causes of childhood obesity
• The food of children
• Junk food of children
• Let's talk about what children do in their free time
• Let's talk about TV and children
• Let's talk about TV and the food of children
The technique used to analyze the information of focus groups was a syntagmatic analysis including the following steps: first, recognizing the subjects and predicates through which discursive objects" and topics were asserted; then, an analysis matrix was generated with the components in their development order: number of paragraph, actor, subjects and predicates, triggering topics and arguments.
The transcript of focus groups allowed, at first in the analysis phase, to separate the colloquial discourse of each of the participating groups; second, all the discourse of focus groups was systematized in an analysis matrix that included number of paragraph, actor, subjects and predicates, triggering topics and arguments; third, the triggers and vectors of the generated information were located, and fourth, discursive subjects and predicates were located in each phrase through which the discursive objects and topics of the generated discourse, building in turn the arguments that gave rise to lineal and multiarticulate schemes.
Results
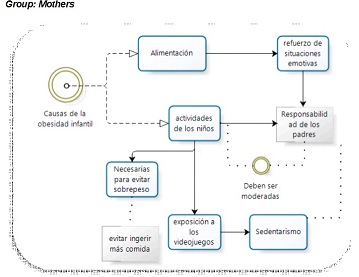
The group discussion started with the childhood obesity trigger and mothers automatically addressed the subject of behavior and eating, which justified that food is used in children as a booster of emotional situations and as a reward for appropriate/positive behaviors: "Well, I think that we always culminate happy or sad moments in life with food; if the kid got a good grade or something like that, we reward him with some food" (Participant 13, female, 42 years, 2 children).
There were clear references to the responsibilities of mothers in regards to the behavior and eating habits of children, landing on their shoulders the absence of monitoring of children's activities, as well as the relationship between the use of new information and communication technologies (ICTs) and sedentary lifestyles.
"They are the reason for consuming more sweets in children, and they also may lead to the lack of exercise and physical activity" (Participant 15, female, 37 years, 2 children).
"Particularly video games, they considerably reduce their interest in going out to play soccer" (Participant 5, female, 39 years, 3 children)
The different responsibilities of parents were addressed regarding the problem, such as controlling entertainment activities and, among the most important, the importance of distributing free time between passive activities (video games) and physical activities.
"I mean exercise, physical activity, practicing some sport, / do not know, take them to swimming classes. Mostly, that they have an extra activity for them to spend their free time in exercising, instead of spending it in eating and, hence, counteract eating" (Participant 7, female, 27 years, 1 child)
Hence, it means dosing activities, / mean, you are going to play with the Xbox, but you are also going out to play soccer, and develop in them, somehow, the fondness for a sport or physical activity" (Participant 8, female, 41 years, 3 children).
Another important element is that the reason for the excessive intake of food in children, leads to a sedentary lifestyle and to anxiety-related compulsive eating. The problems of adults in relation to obesity are reflected in children, including anxiety-related eating behaviors and the control adults assume in regards to physical activity.
"Because most times, it is just the anxiety for having something to such or chew in your mouth, though you are not really hungry" (Participant 2, male, 37 years, 2 children) "For example, / have my ig-y old daughter and my 12-year old son and curiously enough none of them is obese; but it does worry me that they would ever suffer what / have lived, really"(Participant 2, male, 37 years, 2 children) "If you had cake today, try not to eat any in 2 or3 days, / mean, not eating cakes so eft(Participant 8, female, 41 years, 3 children).
Regarding intake and the type of foods that children usually have, there is an evident dislike for "fast food" by mothers. This is extremely related to their food preferences.
"I am not the person who likes toe at pizzas, or burgers, or those types of foods//(Pcrticipcnt 7, female, 27 years, 1 child).
They give their opinion about the typical homemade food that they prefer to cook and, hence, to balance their meals: "I mean, it is the culture that you are developing in them". Besides, in this way they can "mask" healthy food with something innovative and gratifying for children.
"For example, cook some vegetables in the fashion they like better and present them in the dish resembling happy faces or something funny" (Participant 16, female, 38 years, 1 child).
Another important element related to food intake is the impact of advertising and marketing. Participants referred that they are determinant of food intake and its frequency. Besides, it also interferes with their children preference for certain foods which is often determined by the product marketing, instead of by its nutritional value.
"Yes, because TV, when your are watching the ad (and even if your are not hungry then), if you are watching an ice-cream or patty ad, you start craving for one even if you are not hungry"(Participant 15, female, 37 years, 2 children)
"Or, for example, the McDonalds burgers, they simply want the happy meal, and sometimes they do not want the burger, they want the "figurine" and they start insisting on going there. And well, they maybe eat the burger, but it was the ad that encouraged you to go there and purchase /"(Participant 13, female, 42 years, 2 children)
In regards to the trigger of "obese children", mothers relate it to image and provide supporting examples of how babies are visualized pointing out that their "chubby" appearance makes them look "pretty". But, at the same time, they refer to the consequences of developing this disease at such an early age.
"And this is true, and I have witnessed it with my nephews, they both were born really chubby and everybody said "oh, they are really healthy, really pretty" but they are now adolescents and they are still quite chubby" (Participant 7, female, 27 years, 1 child).
An important category is the responsibility of parents for their children eating habits, stressing that parents are the example for their children and assuming their influential role on the their preference or dislike for some type of food.
"For example, I would not dare to speak of vegetables with my daughters (...) and this is maybe because I never instilled the habit of eating vegetables in them, it is like you said, this is the example you should give them so they can see that vegetables are healthy foods and that they are what we are going to eat, or try to eat more often, to lead a healthier l/fe"(Participant 15, female, 37 years, 2 children)
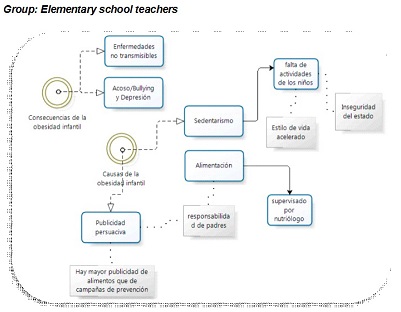
Regarding the quality of life trigger, teachers mentioned the difference between the things that were done in the past and what is done currently, in terms of society temporality, both in terms of physical activities and types of sociability. They pointed out that currently children have no outside-home activities, as compared to the past, due to the perception of insecurity we live with. They also referred to the busy lifestyle of parents that leads to stop paying attention to home activities, such as cooking.
"But today, due to insecurity and to all the negative things that are going on, the parents prefer to leave the children enclosed here and they have everything they need and cannot go out on the street" (Participant 26, female, 31 years)
"I mean, let's say that the mom works, and then the lifestyle is busy, busy, and so she thinks: well, I would simple prepare something practical, and would buy this; I would buy this on my way home for them to eat" (Participant 18, female, 42 years)
Regarding the impact of mass communication media, they mention advertising and consider it as extremely persuasive, "including a subliminal message"that adds up to the permissiveness of parents.
"And the parents, in order to avoid quarreling, simply say yes, buy it, buy it for him" (Participant 16, female, 47 years)
As to the things that make children happy, the emotional effect of sweets was mentioned, but in relation to the consequences of obesity and, in its presence, the harassment or "bullying" that obese children encounter at school, which lead to social interaction issued in these children.
"Well, if they are obese or chubby kids, there are other kids that make a lot of fun of them, and there starts bullying" (Participant 28, male, 26 years)
In regards to the disease risks, they stated that feeding should be supervised by a dietitian, but this means expenses that many families cannot pay for. They also mentioned related disorders such as hypertension, diabetes, high cholesterol levels, stress, and particularly bullying and depression.
"Indeed, because they sometimes have some tendencies, even suicidal tendencies, because they think: everybody hates me or thinks I am ugly"(Participant 18, female, 42 years)
In relation to obesity prevention, teachers noted the existence of prevention campaigns in mass communication media. However, they stated that they have no impact, since the advertising campaigns on junk food outnumber them and have a greater effect. Nevertheless, they also justify the existence of this type of products in the market since the companies that manufacture them give jobs to many persons. They recommend moderating their intake and this is the job of parents.
"If companies like "Sabritas"or ''Coke"disappeared, how many people are paid their income by these companies? Everything in good measure. " (Participant 27, female, 52 years)
"Sometimes, kids refuse their meals because they have been eating chips or cookies, and many parents, to avoid quarreling or because the kid is crying, give him the chips or cookies, instead of conditioning behaviors and saying: eat your food" (Participant 28, male, 26 years)
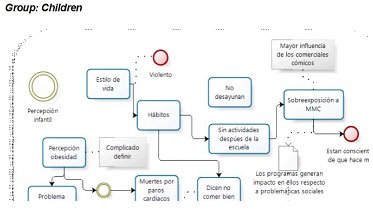
In relation to the quality of life trigger, there was a consensus among children as to describing their family situation as conflictive or negative. They are happy when there are no problems, yelling at home, and they are sharing a good laugh with the family.
"If my dad does not drink and goes to work, I am happy" (Participant 41, boy, 8 years)
In the case of "children's food", the kids mentioned as their favorite the barbacoa tacos (traditional dish of Nuevo León) and golden fried tacos. They do perceive that the basic basket food, such as eggs and beans, have increased their price and become expensive, such as the eggs and beans.
"Only the rich people eat eggs"(Participant 36, boy, 11 years)
"Even beans are too expensive"(Participant 37, girl, 11 years)
Defining obesity was difficult for children. They referred to "a chubby friend" and made jokes about him, but they indeed identify that it is "a weight problem and excessive eating."
"I have a cousin who is really fat because he is given Coke only, and my cousin's friend is also fat"(Participant 43, girl, 10 years)
Besides, they pointed out that they normally take home-prepared food to eat at the school break and it is usually sandwiches. They said that what they really like to eat is fried snacks (chips), sweets and "junk food, in general because it is practical, "but they are perfectly aware that these foodstuffs provide no health benefits.
There is a consensus among children that they have no breakfast before leaving to school. "I almost have no breakfast because I do not like /'"(Participant 32, girl, 11 years)
Regarding their leisure, it must be highlighted that they spend a long time lying, watching TV, or sitting before a computer engaging in social networks or browsing the internet. In their own habit evaluation, they are aware that they "do note at well" or eat excessively. They also know that spending time constantly in a lying position while consuming mass communication is bad for their health. One of the activities that girls like is dancing.
"When I get back home, my sister makes me wash dishes and then I go on Facebook and I almost make no exercise at a/l"(Participant 44, boy, 11 years) "I dance, because it is bad to stay lying and connected" (Participant 40, girl, 12 years)
In regards to advertising, they remember the characteristics of funny ads and refer that most of them are related to food. They places they like to go better for lunch are the franchises such as KFC, Burguer King, and others where buffets are offered.
"I like the ad with the emperor, where he shouts: guards, guards!"... (Participant 32, girl, 11 years)
"Ah, yes, and then he says it is very good'ffParticipant 33, boy, 11 years)
When the subject of obesity risks was addresses, they mostly spoke about cardiovascular diseases, mainly "heart arrest", and only one mentioned diabetes. There is a considerable reference to the experiences of people they know who have suffered heart arrests/attacks or to cases they have seen on TV.
"Yes, there was once a story in the program 'Como dice el dicho' (As the saying goes, of a man that always took his son to eat at a taco street stall and he fell there in the middle of the street and he was really sick, but he would not understand and died later" (Participant 40, girl, 12 years)
They are aware that, to prevent obesity, there must be physical activity and medical supervision by a dietitian and a psychiatrist.
"Visiting a dietitian to be given a good diet, and also visiting a psychiatrist if they have problems quitting" (Participant 37, girl, 11 years).
In relation to the trigger "social perception of obesity", it is noteworthy that they perceive it as problem that is out there and that those who suffer it, do not think they have it, but they do identify it as an eating problem: "those kids do not think that they have a problem"(Participant 36, boy, 11 years).
Discussion
Perception is conventionally defined in social psychology as "the cognitive process of consciousness consisting on recognition, interpretation and significance to form opinions regarding the sensations obtained from the physical and social environment, in which other psychic processes are involved, including learning, memory and sumbolization."20
The social perception of the three agents studied was different in the five semantic fields covered. However, if connections are established among the three points of view, a general social perception can be mapped regarding childhood obesity.
Experts in nutrition devoted to public health have always displayed a very special interest in finding indicators that are not expensive to study and easily applicable in field works, as well as adequate for identifying the populations at risk of malnutrition, either due to eating deficit or excess.21 It is under the premise that the social perception of obesity must be studied that an effective health communication strategy.
To make a general mapping of this social perception, groups were formed with key agents that constantly interact with the target population of this research. Hence, mothers were proposed, since in Mexico they are usually in charge of their family and children eating habits, as well as elementary school teachers since they perform as the observers of the child situation and, at the same time, have contact with mothers, therefore occupying an objective position regarding the problem.
The general results indicate that regarding the quality of life of children, elementary school teachers identify the children that have no activities outsider home, due to the perception of insecurity that prevails in this state of the republic, and which leads to inactivity in children. They also identify other factors, such as the busy lifestyle that parents that work or have too many activities have to cope with. They do not have time cooking and there is only enough time to buy some fast food on the go, which in turn prevents monitoring an adequate nutrition. Besides, it is argued that, due to this same lifestyle, it is not possible to supervise the children's activities and rather prefer to leave them enclosed at home watching television. This version agrees with that of children who say that, after school, they spend their time lying in front of the TV or sitting before a computer browsing the internet or connected to Facebook. This makes reference to the study of Cano,22 who points out that most students know that physical activities and diet are important, but do not acknowledge the management of stress. Children must be explained that sports and other activities would help them interact better with their environment and promote physical activities.
There is a very different social perception among groups in regards to the quality of life and happiness of children. Parents and teachers refer to the food rewarding processes as a reason for happiness, while children refer to family harmony as the main reason for happiness (they point out that they enjoy considerably when sharing a good laugh or chat with the family). This interaction with the environment from the perspective of children is decisive for their development since, as Aranda states,23 children interact with the environment and receptors of environmental forces. However, the discourse of children allows perceiving that their environment is not positive, full of constant family conflicts, yelling, fights and alcoholism.
It is interesting that some derivations are not found as such in the subject of obesity, though they are part of social discourse. For example, in relation to the conditions that lead to inactivity, it is mentioned by adults that violence is found outside home, while children see violence within the family and it prevents their full development as persons.
This may be justifiable because the act of perception is not a linear process but quite the opposite, since it dynamics implies constant interaction between the individual and the social, and nourishes from the social assessments and rules.20
The busy lifestyle is also perceived in relation to the busy lifestyle. Mothers have no time for cooking and even let their children to go to school without any breakfast. This may also be related to the fact that children spend all the time they want lying before the TV, which has been extensively documented as an environmental factor that has contributed substantially to the increase in the prevalence of childhood obesity.11' 10 18
The social perception of childhood obesity is different for the three groups. In the case of mothers, a "chubby" child is synonymous with being "pretty and healthy". However, they detect there is an obesity problem only when children reach adolescence or even adulthood. If the mothers are overweight, they want to prevent their children from "suffering" the same "disease". For the group of teachers, the social perception of childhood obesity is identified with depression and bullying. They blame the disease for making children insecure and laughed at by other kids for not being able to participate in physical competitions, situations that become so extreme at times that lead to low self-esteem problems and even suicidal tendencies in the overweight or obese child. Children perceive obesity as foreign subject to which they have no relation with. Therefore, defining obesity is not easy for them and they simply explain it as problem derived from overeating.
In regards to the social perception of the mother and teacher groups in relation to the influence of mass communication media in childhood obesity, these two groups agree that the advertisement of foodstuffs is highly persuasive and leads to consumerism. Conversely, for children part of their happiness is present in the influence of mass media, since they refer to funny ads as the most pleasant and related to their intake preferences/ habits. It is clear that children remember the stories they see in television, since they use them as references to explain or describe their perception of social problems.
Conclusion
Eating behavior refers to the set of actions that determine the relationship between human beings and their food. It is generally accepted that behaviors before food are acquired through the direct experience with food in the family and social environments, and by imitation of models, availability of food, social status, emotional symbolisms and cultural traditions.10
It is important to determine the social perception of food intake and obesity in relation to the quality of life that individuals pursue, i.e., in relation to well-being or, as children call it, happiness. To this end, it is essential to link the social and cultural values that determine the relationship between children and adults, since the formation of impressions and rewarding processes are so diverse and lead to adverse outcomes, including obesity.
The mechanisms to modify said behaviors must include the following elements: 24 1. Familiarity, by using stimuli typical to the specific culture to develop perceptual mechanisms; 2. Functional value, including the environment properties that develop stimuli selectivity, predisposition, or rejection mechanisms, and 3. Communication systems that use symbolic elements to convey the relevant meaning and sense.
Finally, the social perception emphasizes both the social and symbolic interaction processes. Hence, the objective of the communication strategy must pursue the associated factors for the prevention of obesity by using the symbolic elements of groups, while taking into account the senses and meanings that, from the social perspective, are related with the basic stimuli to unleash behaviors related to obesity.
References
1. Nguyen, N., Champion, J. K., Ponce, J., Quebbemann, B., Patterson, E., Pham, B., & Favretti, F. A review of unmet needs in obesity management. Obesity surgery; 2012; 22(6), 956-966.
2. Sassi, F. Obesity and the economics of prevention: fit not fat. OECD. 2010.
3. UNICEF. Salud y nutrición. Available at: http://www.unicef.org/mexico/spanish/17047.htm. [Last Accessed 20 de junio de 2013].
4. COEPO Consejo Estatal de Población de Jalisco, Diez Problemas de la Población de Jalisco: Una Perspectiva Sociodemográfica, 2010. Disponible en http://coepo.app.jalisco.gob.mx/PDF/LibroDiezproblemas/Capitulo1.pdf consultado el 19 de abril de 2013.
5. Liria, R. Consecuencias de la obesidad en el niño y el adolescente: un problema que requiere atención. Rev. Perú. Med. Exp. Salud pública. 2012; 29(3), 357-360.
6. Ponce, G., de León, P., Acosta, M. E. H., Torres, M. A. A., & Núñez, A. A. Obesidad y tejido adiposo. Salus. 2010; 11(2).
7. COEPO. Consejo Estatal de Población de Jalisco, Diez Problemas de la Población de Jalisco: Una Perspectiva Sociodemográfica, 2010. available in http://coepo.app.jalisco.gob.mx/PDF/LibroDiezproblemas/Capitulo1.pdf consultado el 19 de abril de 2013.
8. OMS. Estrategia mundial sobre régimen alimentario, actividad física y salud. Retrieved. 2013; from http://www.who.int/dietphysicalactivity/childhood_why/es/
9. Bhattacharya J, Sood N. Who pays for obesity? J Econ Perspect. 2011; 25:139-58.
10. Morales, M. J. Cuando Barbie se come a Garfield. Publicidad y alimentación: niños obesos buscando la perfección del cuerpo adulto. Trastornos de la conducta alimentaria. 2006; (3), 245-263.
11. Hidalgo, C. G., & Samur, E. A. Regulación de la publicidad televisiva de alimentos para prevenir la obesidad infantil. Archivos latinoamericanos de nutrición. 2011; 61 (3).
12. Tapia López, L. G., & Sánchez Alejandro, A. Percepción de la imagen corporal que tienen las madres respecto a sus hijos. Mimeo 2010.
13. Barrientos-Pérez, M., & Flores-Huerta, S. ¿Es la obesidad un problema médico individual y social? Políticas públicas que se requieren para su prevención. Bol Med Hosp Infant Mex, 2008; 65(6), 639-651.
14. Kuri-Morales, P., & Chávez-Cortés, C. La transformación del sistema y los espacios de la salud pública. Órgano Oficial de la Academia Nacional de Medicina de México, AC. 2012, 148, 509-17.
14. García-García, E., De la Llata-Romero, M., Kaufer-Horwitz, M., Tusié-Luna, M. T., Calzada-León, R., Vázquez-Velázquez, V. & Sotelo-Morales, J. La obesidad y el síndrome metabólico como problema de salud pública: Una reflexión. Salud pública de México. 2008; 50(6), 530-547.
16. OMS. Estrategia mundial sobre régimen alimentario, actividad física y salud. Retrieved. 2013; from http://www.who.int/dietphysicalactivity/childhood_why/es/
17. Valera, S., & Pol, E. El concepto de identidad social urbana: una aproximación entre la psicología social y la psicología ambiental. Anuario de psicología. 1994; 62(3), 5-24.
18. Travé, T. D., & Visus, F. S. V. Obesidad infantil: ¿un problema de educación individual, familiar o social?. Acta Pediatr Esp. 2005; 63, 204-207.
19. Azteca Noticias, Tiene Nuevo León primer lugar en obesidad infantil. 06-Abril. (Info7.mx). Consultado el 03 de julio de 2013, available in: http://www.info7.com.mx/a/noticia/383860
20. González, A. Percepción de la calidad de vida urbana en las ciudades de la frontera: Norte de México. Población, urbanización y medio ambiente. 2008; 15.
21. Madrigal-Fritsch, H., Irala-Estévez, J. D., Martínez-González, M. A., Kearney, J., Gibney, M., & Martínez-Hernández, J. A. Percepción de la imagen corporal como aproximación cualitativa al estado de nutrición. Salud pública de México. 1999; 41(6), 479-486.
22. Cano, Juan Manuel Muñoz; Melzer, Jorda Albarrán; Salazar, Teresita del Niño Jesús Maldonado. Competencias para la promoción del estilo de vida saludable. Horizonte sanitario, 2014; 6 (3): 4-11.
23. Aranda Alfredo Briones, et al. Prevalencia de estrés en escolares de Tuxtla Gutiérrez Chiapas, México y factores familiares asociados. Información psicologica, 2015; 108: 19-30.
24. Tajfel Social and cultural factors in perceptions. The handbook of social psicology., Lindzey, G y Aronson. 1969; E. 3, cap. 22.