Health Economics
Usage profile and out-of-pocket health expenses of patients visiting a prívate medical office to receive dental care treatmens. Reforma, Chiapas, 2015.
Perfil de uso y gastos de bolsillo de pacientes que acuden a una consulta privada de estomatología. Reforma, Chiapas, 2015.
Jonatan flores morales! 1, Jeannette Ramírez Mendoza 2, Manuel Higinio Morales García3
(1) Private Dental Surgeon, specializing in Orthodontics, Master in Public Health.
(2) Dental Surgeon, specializing in Odontopediatrics, Professor and Researcher of the Academic Division of Health Sciences.
(3) Dental Surgeon. Master in Population Health Sciences, Doctor in Education Sciences, Professor and Researcher of the Universidad Juárez Autónoma de Tabasco.
CORRESPONDING AUTHOR: Manuel Higinio Morales García. Coordinación de Cirujano Dentista, División Academica de Ciencias de la Salud de la de la Universidad Juárez Autónoma de Tabasco. Av, Gregorio Mendez Magaña No. 28-38-A, Col. Tamulte, CP. 86150 Villahermosa, Tabasco, México. E-mail: mchiginio@live.com.mx
Original received May 12, 2015
Accepted August 1st, 2015
Abstract
Objetive. To describe the social and labor characteristics, usage profile, satisfaction and dissatisfaction of users in regards to the out-of-pocket health expenses of patients enjoying social security when visiting a private dentistry office. Material and method: An observational, analytical study was conducted in a population of 84 private practice users. The sampling was simple random, using a questionnaire that measures the use and out-of-pocket dentistry expenses. Results: The surveyed patients receive a wage, have a formal employment, and are affiliated to a social security institution. Regarding the procedures undertaken to receive dental care in the social security institution, 60% of the users were dissatisfied, 41.7% answered that they never received the adequate treatment, and 78.6% stated they were not satisfied. However, in private dental offices, 56% of the patients stated they were completely satisfied with the treatment received and with the promptness with which they received care and 100% stated they would definitely return to receive dental care. Conversely, over 70% was dissatisfied with the high cost of treatments, one third was not satisfied with the amount paid or the treatment provided at the private offices, and 44% categorically stated that the usage of private care had a considerable impact on their economy. Conclusions: The patients affiliated to a social security institution do not seek dental care in the dental area due to the procedures they must follow. The users rather seek private care due to the promptness in service, the dentistpatient relation, the information received, despite the high cost of the treatment and its direct impact on their personal and family economy.
key words: Usage profile, Out-of-pocket spending, Dental services .
Resumen
Objetivo: Describir las características sociolaborales, el perfil de uso, satisfacción e insatisfacción de los usuarios con relación a los gastos de bolsillo en pacientes que cuentan con seguridad socialy acuden a consulta privada de Odontología. Materiales y métodos: Se realizó un estudio observacional, analítico, en una población estudiada de 84 usuarios que acudieron a consulta privada. El muestreo fue aleatorio simple, se aplicó 1 cuestionario, que mide el perfil de uso y el gasto de bolsillo. Resultados: Los pacientes encuestados, perciben un salario y cuentan con un trabajo formal; y están afiliados a una institución de seguridad social. El 60% de los usuarios se sintió insatisfecho con los trámites que debió realizar para recibir atención de estomatología, el 4i,7%respondió que nunca le brindan el tratamiento adecuado y el 78,6% declaran que no. Sin embargo, en los servicios de atención privada de estomatología, el 56% expresó máxima satisfacción con la realización del tratamiento realizado y la rapidez con que reciben la atención, el 100% de ellos si regresarían a recibir atención de estomatología. En contraste, más del 70% se sintió insatisfecho por los elevados costos de los tratamientos, la tercera parte se mostró insatisfecho con el monto del pago que debió hacer por el servicio de odontología que le prestaron en la consulta privada y el 44% afirmó categóricamente que el uso del servicio privado afectaba mucho su economía. Conclusiones: Los pacientes afiliados a su institución de seguridad social no acuden a recibir atención del área de estomatología por los trámites que tiene que realizar, los usuario prefieren acudir a consulta privada por la rapidez de la atención, y por la relación odontólogo-paciente, la información que reciben, aun con los elevados costos que pagan para la realización de sus tratamientos y el impacto directo en su economía personal y familiar.
Palabras clave: perfil de uso, gasto de bolsillo, Servicios odontológicos
Introduction
Mexico is among the countries with the highest frequency of oral diseases, with dental caries and periodontal diseases as the stomatognathic system problems that have historically affected the population mostly. According to WHO reports, the prevalence of these two diseases in the country's population is of 90 and 60 %, respectively, having a negative impact on the quality of life of people.1, 2
The Mexican health system comprises two sectors, public and private. Within the public sector, there are the social security institutions which include, among others, the Mexican Institute of Social Security (IMSS), Institute of Security and Social Services for State Employees (ISSSTE), Petróleos Mexicanos (PEMEX), Secretary of Defense (SEDENA), and Secretary of the Navy (SEMAR). There are other institutions and programs that take care of the population that has no social security, such as the Secretary of Health (SSA), State Health Services (SESA), Program IMSS-Oportunidades (IMSS-O), and the People's Health Insurance (SPS)].3
The private sector comprises insurance companies and healthcare providers that work in private practices, clinics and hospitals, as well as the providers of alternative medicine.
However, the oral health services are negatively affected by the scarcity of public financing programs, the high cost of technology, the workload of the professionals in the field and their attitude, as well as the inadequate level of priority given to the most vulnerable population and the services devoted to this type of care. Consequently, a considerable proportion of the patients visiting the public oral health services are dissatisfied and, paradoxically, would rather spend their mostly limited resources in private dental services to evidence their dissatisfaction.4
Oral health is a major component of the general health and quality of life of people and its related diseases still represent a worldwide public health issue.
Their high prevalence and incidence place them as the most common chronic diseases and the high costs of their treatment translate into profound disparities in terms of access and care for the most vulnerable populations, hence becoming a considerable challenge for health systems. The most common oral diseases are dental caries and periodontal diseases. By way of example, 60%-90% of school-age children suffer dental caries.5, 6
The traditional curative dental care represents a major economic load for many high-income countries where 5%-10% of the public sanitary spending is related to oral health. Guaranteeing basic services in this area involves the investment of numerous resources given the complexity of treatments which require equipment, materials, adequate energy, water, and lighting supply, not to speak of the development of professional competences and the systematic requalification of professionals given the frequent technological changes making of this specialty a very costly one that requires high efficiency levels in order to provide coverage to the population that needs it.
Therefore, it is a undeniable fact that the health sector expenses constantly increase and that these expenses represent a negative load for both the public sector and the private user budgets.
The family income is a determining factor of the prevalence of oral diseases, an association that is developed as a negative correlation between both, i.e., the higher the family income, the lower the risk to suffer gingivitis. Such claim has been confirmed by recent studies reporting a highly significant association between both variables.
Something similar happens with the family income and the time elapsed since the last visit to the dentist since an individual that does not have enough economic resources to use the private care services, is forced to go to public care facilities center that are characterized for offering palliative therapeutic options that have a very low impact in solving the patient's oral health problems.
In other words, the individuals enjoying a better income can go to a private practice and ask for medical care even where there is no pain or emergency since they have the purchasing power to do so, to receive care that is mostly focused in prevention in most cases.7
Several studies have quantified the social consequences of disease through the limitations it imposes on daily activities and quality of life. However, the study of the health status has included primarily the spectrum of severe and chronic disorders and has paid little attention to the social impact of oral disease, i.e., oral problems have been measured with an emphasis on tissue pathology and with a limited recognition of their general implications on the health and life of individuals.
Oral diseases are progressive and cumulative and become complicated overtime, affecting the ability to eat, appearance and ways in which people communicate.
The oral cavity is not free of the effects of aging and several attempts have been made to establish links between oral diseases and other disorders, and the relationship between chronic degenerative diseases, such as diabetes mellitus and hypertension, with the modifications in the oral soft and hard tissues has been studied. Dental caries and periodontal disorders are the main causes of tooth loss in the population.8
It is proven fact that oral health is not given the same level of priority as the remaining services in health systems, and neither does the population that has no economic resources attaches the same importance to oral diseases, despite their physical and psychological impact. A poor oral health has an influence on self-esteem and personal growth, on the performance of daily activities, such as looking, chewing and tasting food, speaking and promoting social interaction, including the perception of the own well-being since early childhood and all along life.
Given their high morbidity, oral diseases have a considerable demand for care services and exceed the installed resolution capacity. To reverse this situation, it is necessary to improve the infrastructure of said services and implement preventive measures that could have an impact on their incidence. This is particularly relevant under the current conditions where there is a high level of population aging that increases the demand for curative services in relation to dental caries, periodontal diseases, rehabilitation treatments, such as prosthesis, and specialized attention, as in the case of oral cancer.
However, though it is essential to increase coverage to reach the greatest possible number of vulnerable groups, it is also true that the resources will always be insufficient if the need to improve the quality of care is not taken into account. 9, 10
Materials and methods
A partial economic evaluation, observational, analytical study was conducted analyzing the dental care out-of-pocket expenses in a private dental office in the municipality of Reforma, Chiapas.
The information was gathered through a questionnaire called Survey of usage profile and out-of-pocket expenses of clients that visited a private dental office.
The surveyed patients were n= 84, had a formal employment, received a wage and were affiliated to a social security institution.
The collected data were entered in a database designed in Excel (Microsoft) and processed with the statistical software package SPSS (StatisticalProduct and ServiceSolutions), version 2.0. The association among the studied variables was determined using the statistical Chi-square independence test, with a significance level of 0.05.
Results
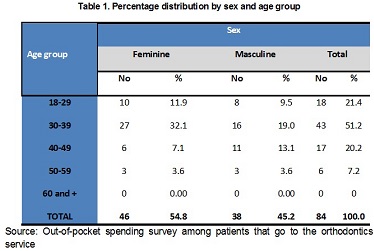
The highest proportion of interviewed persons had a relationship with a steady partner (65.5%), with or without legal ties, either married or cohabiting, and 33.3% were single; 92.9% were working at the time the survey was conducted and the remaining were retired.
In regards to age group, the 30-39 year old, masculine group stands out as the group with the greatest percentage of patients requesting service.
Regarding services, 60% was dissatisfied with the procedures to be completed to receive care; 77.4% was not satisfied or extremely dissatisfied with the availability of materials; 67.9% considers that the care received was poor or very poor, while 78.6% is not willing to return to the dental services offered by their labor organization.

The most demanded services were those of specialties, mainly prosthesis followed by orthodontics, as well as other treatments such as dental treatments and extractions.
As to private care, 60.7% have attended on average twice a month; 96.5% was very satisfied with the procedures to be completed to receive care. In regards to material availability, 98.8% was satisfied and 56% was extremely satisfied; 44% was very satisfied with both the medical and personal treatment received from the dental surgeon, 77.4% mentioned the high treatment costs, and 100% would return to receive treatment in a private medical office.
Discussion
The analysis of oral health is one of risky factors to handle in health research. The organization, quality, and efficiency of services depend on its progress, as well as on the population's health education, among other essential aspects.
To the extent that patients learn to take care of their stomatognathic system and, particularly, inasmuch as they count with the means to achieve it, meaning affordable oral health services, with qualified staff and appropriate for the culture, they may be able to build a protective wall against these diseases that have a detrimental effect on their quality of life and general health, from childhood to old age, as well as in their selfesteem, ability to eat and nutrition.
Positive self-perception mechanisms in terms of health must be recovered in order to organize the human and material resources in favor of communities as a whole because "disorganization becomes self-destructive."11
The fragmentation of the individual, as well as the biases in the care of the population must be consciously avoided by all specialists who must also be trained and educated by each other to provide the assertive orientation that patients need.
Overcoming the issue of knowledge fragmentation involvesdeveloping multidisciplinary and interdisciplinary diagnostic integration efforts since, regardless of how well the dental surgeon may take care of teeth, gums, and their basic connections with other body organs and systems, he would hardly achieve the best results if he faces problems of disqualification, invisibility of his work, or even absolute disregard for his efforts. A broad connection must exist with and within the other physicians, specialists, and healthcare professionals who share the responsibility of safeguarding the health of the human species.
There is an urgent need to train the health staff in the maintenance of the integral individual and social health, from the very family nucleus. The goal is to establish the required approach to health promotion, based on analysis of its determining environmental, cultural, economic, social, and political factors, among others.
The Mexican Official Standard perceives health education as "the teaching and learning process that allows, through information exchange and analysis, the development of abilities and the change in attitudes aimed at modifying behaviors to take care of the individual, family, and collective health."12
Conclusion
In the study group, the mostly represented institutions were Petróleos Mexicanos, the Mexican Institute of Social Security and the Institute of Security and Social Services for State Employees, powerful institutions in terms of resources and prestige, in contrast to the unfavorable opinion given by the surveyed patients in regards to the dental care services they provide.
Patients use frequently the dental services of their institution, once a month on average, while those using private services visited them at least twice a month, which speaks of a more prolonged treatment and systematic care.
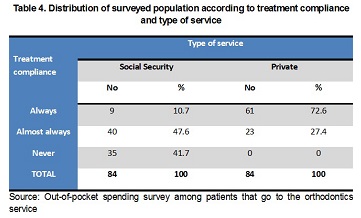
These patients showed a higher degree of satisfaction with the private services and awarded a higher level of pertinence to the applied treatment, and all the surveyed persons considered that this type of services always or almost always solve the problem they visited for which is an indicator of care accessibility and quality.
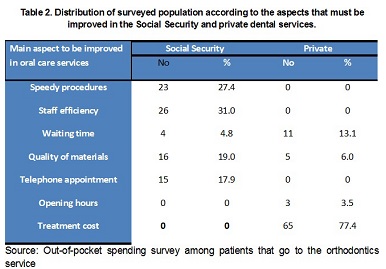
A marked difference is also clear in terms of the aspects to be improved in both services. The two main factors to be improved in the private sector are a reduction of costs and waiting time, while in their social security institution, they were mainly the staff efficiency and speed of the procedures.
The out-of-pocket expenses of those attending a private clinic were considerably high and included the direct care, diagnostic testing, medications and transportation costs. Other expenses included the time spent in transport as well as the discounts or loss of wage due to absence of work of the patient, his accompanying relative or both.
Even though its sample was small, the study showed the magnitude of out-of-pocket expenses and their impact on the personal and family economy of those who use private dental care services due mainly to the weaknesses that, according to them, pervade in the social security institutions they are affiliated to in terms of accessibility and quality of dental care.
References
1. Salud Bucodental. Nota informativa N° 318. Febrero de 2007. Available in en:http://www.who.intmediacentre/factsheets/fs3i8/es/.
2. Organización Panamericana de la Salud / Organización Mundial de la Salud. Salud en las Americas. Panorama regional y perfiles de país. Publicación Científica y Técnica No. 636. Washington, DC: OPS, 2012.
3. García JF. Financiamiento de la salud en México. Pasos hacia una política de estado en salud. Pág. 249-267. In: Gálvez AM, García A. Resultados de investigación en economía de la salud. Ed. Ciencias Médicas. La Habana, 2014.
4. Murrieta J, Juárez L, Linares C, Zurita V, Meléndez A, Raquel C, et al. Prevalencia de gingivitis asociada a la higiene oral, ingreso familiar y tiempo transcurrido desde la última consulta dental, en un grupo de adolescentes de Iztapalapa, Ciudad de México. Rev. Medigraphic [en línea] Vol. 65, September - October 2008. Available in : http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=Si665-ii462008000500006.
5. Murrieta J, Juárez L, Linares C, Zurita V, Meléndez A, Raquel C, et al. Prevalencia de gingivitis asociada a la higiene oral, ingreso familiar y tiempo transcurrido desde la última consulta dental, en un grupo de adolescentes de Iztapalapa, Ciudad de México. Rev. Medigraphic [on line] Vol. 65, September - October 2008. Available in: http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=Si665-ii462008000500006.
6. Marie F, González E, Gómez O, García D, Arreola H, Barraza M, et al. Hacia la cobertura universal en salud: protección social para todos en México. Salud pública de México. [en línea] vol. 55, no. 2, March - April 2013. Available in: www.scielo.org.mx/scielo.php?pid=S0036-36342013000200013
7. Pontigo A, Medina C, Márquez M, Vallejos A, Minaya M, Escoffié M, et al. Utilización de servicios de salud bucal. Gaceta Médica de México. [on line] 2012; 148:218-26.
8. Sánchez M, Román M, Dávila R, Pedraza A. Salud bucal en pacientes adultos mayores y su asociación con la calidad de vida. Revista de Especialidades Médico-Quirúrgicas 20ii;[on line] 16(2):110-115. Available in: www.redalyc.org/pdf/473/47319326010.pdf
9. Medina C, Villalobos J, Márquez M, Vallejos A, López C, Casanova A. Desigualdades socioeconómicas en la utilización de servicios de salud bucal: estudio en escolares mexicanos de 6 a 12 años de edad. Cad. Saúde Pública [on line] Dec. 2009. vol.25 no.12 Río de Janeiro Available in: http://www.scielo.br/scielo.php?pid=Soi02-iiX200900i200009&script=sci_arttext
10. Medina C, Pontigo A, Pérez E, Hernández P, De la Rosa R, Navarete J, et al. Principales razones de extracción de dientes permanentes en una muestra de adultos mexicanos. Revista de Investigación Clínica [on line]March - April , 2013 Vol. 65(2^141-149. available in: revistas.curnvirtual.edu.co/journals/index.php/cienciaysalud/article/.../42
11. Ruiz H, Herrera A. La prevalecía de periodontopatías y algunos factores de riesgo en el adulto mayor. Revista Cubana de Investigaciones Biomédicas.[on line] 2009^8(3) 73-82. Available in: scielo.sld.cu/scielo.php?script=sci_arttext&pid=So864
12. Programa de promoción y atención a la salud bucal en Chiapas. Available in: http://salud.chiapas. gob.mx/Portal/noticias/salud-establece-programa-de-promocion-y-atencion-a-la-salud-bucal/